
30. The Challenges andBenefits of Digital and Online Learning in Recovery Colleges
Written by Sara Meddings, Waldo Roeg, Kirsty Giles and Ashleigh Charles
With thanks to Joanna Peckham (Dorset Healthcare University NHS Foundation Trust) and Jane Carey (Dorset Mental Health Forum), Joanne King (Tees, Esk and Wear Valley NHS Foundation Trust Recovery College Online), Linda Birt (Leicester University), Catherine Briand, Myreille Bédard, Martine Vallarino and Filippo Rapisarda (Université du Québec à Trois-Rivières and Centre d’apprentissage Santé et Rétablissement, Montréal, Canada); Louise Patmore (Sussex Recovery College, Sussex Partnership NHS Foundation Trust and NHS Sussex (Sussex ICB) ), Nelida Senoran Martin (Sussex Recovery College, SPFT) Bryher Bowness (South London and Maudsley NHS Foundation Trust, SLaM), Mark Dalgarno (SLaM), Iris Dearne
(Inclusion Thurrock Recovery College, MPFT NHS Trust), Oliver Kane, Betsey Walker and Bev Howards (Midlands Partnership NHS Foundation Trust), Sue Williams
(Imroc), Rachel Perkins (Imroc), Emma Watson (Imroc) and Jane Rennison (Imroc).
With thanks also to members of the Imroc Recovery College Learning Set whose discussions have informed the development of the paper throughout; to attendees at the Sussex Recovery College Ten Year Celebration Day, and everyone else who has informed the writing of this paper.
Introduction
A Digital Recovery College is one that delivers some or all of its activities through digital and online methods, while maintaining the core Recovery College principles of co-production and co-learning, recovery orientation, adult learning or education, and inclusivity.
The shift to online learning during the Covid-19 pandemic marked a turning point for Recovery Colleges. While the move to online learning was initially a necessary response to social isolation and lockdowns in early 2020, this became an opportunity to rethink how Recovery Colleges could diversify their course delivery methods. By adopting digital platforms such as Zoom, Microsoft Teams, and
e-learning, alongside hybrid classroom models, Recovery Colleges began to rethink the traditional in-person approach. While face-to-face, co-produced, and recovery-focused teaching remains a central part of Recovery Colleges, the introduction of new online options has broadened access and opened new learning environments. What started as a temporary measure to reach students during periods of restricted in-person teaching has led to changes in student demographics and needs, prompting Recovery Colleges to consider how best to meet the needs of a diverse community.
This briefing paper explores how Recovery Colleges have adapted their teaching methods to include online learning offers, focusing on the experiences of both students and staff during this transition. It examines the unique benefits and challenges of online learning, framed through the lens of accessibility, and the core features of Recovery Colleges: adult learning, co-production and co-learning, and a recovery orientation. We highlight the need for flexibility in learning approaches, acknowledging that there is no one-size-fits-all solution. We begin to address some of the issues with online approaches and emphasise how diverse learning options can create new opportunities to broaden access and ensure that Recovery Colleges are accessible for all.
What are Recovery Colleges?
Recovery Colleges are now an established part of the mental health system and offer co-produced educational courses on recovery and wellbeing, mental health and long term physical conditions. Recovery Colleges focus on co-production
and co-facilitation by experts by lived experience (usually peer trainers and also students) alongside subject matter experts (for example, clinicians, public health professionals, employment advisors). Co-production is key to all aspects of Recovery College development and operation from staff recruitment and student enrolment systems to course design and delivery, from governance systems to evaluation.
The main defining features of Recovery Colleges that contribute to positive outcomes for students are the empowering recovery-oriented environment, co-production and co-learning, inclusiveness and adult learning education principles (Perkins, et al., 2018; Toney et al., 2018). All voices are equal; ‘technical’ and ‘lived experience’ have equal validity and significance. The key defining features of Recovery Colleges are shown in Figure 1.
Recovery College curriculums offer education to support understanding health and well-being across and within communities. Co-production in Recovery Colleges centres around sharing power between experts by profession and experts by lived experience of mental health problems or distress. This moves away from traditional health models in which expertise is held solely by professionals.
The first Recovery College opened in London, England in 2009, and several hundred now operate across 28 countries (Perkins et al., 2018; King & Meddings 2019; Hayes et al., 2023). Research and evaluation show that Recovery Colleges are popular and students are generally highly satisfied. Recovery Colleges are associated with students achieving personal recovery goals and socially valued goals; developing knowledge and skills, and improving recovery, wellbeing, and quality of life; along with changes in service providers’ practices and reduced service use and costs
(Meddings et al., 2015; Perkins et al. 2018; Toney et al., 2018; Crowther et al., 2019, Thériault et al., 2020; Briand et al., 2025; Ronaldson etal. 2025 pre-print;).
However, most research into Recovery Colleges is from Western, Educated, Industrialised, Rich Democratic (WEIRD) countries and cultural adaptation is needed in implementing Recovery Colleges across diverse contexts and cultures (Kotera et al., 2024; Kotera et al., 2025). We also need to understand the differences between online and face-to-face cultures and adaptations in developing high-quality digital Recovery Colleges.
Six Defining Features of Recovery Colleges
They are based on educational principles (Adult Learning)
Coproduction, co-facilitation and co-learning lie at the heart of their operation (Co-production)
They are recovery-focused and strengths based (Commitment to Recovery)
They are progressive (Tailored to the individual)
They are integrated with their community and with mental health services; and form a bridge between the two (Community focus & Social connectedness)
They are inclusive and open to all (Equality)
Perkins et.al. (2018)
Recovery Colleges were initially developed in the field of mental health and wellbeing. They have expanded to include courses and workshops for those with a range of physical health conditions, such as cancer or diabetes, and people facing a variety of life challenges, such as bereavement or retirement. They move away from a system which is “hospital-centric, detached from communities and organises its care into multiple, fragmented siloes” (Department of Health and Social Care, DHSS, 2025, p.9) and move to a more person-centred service which brings together health, social care and voluntary community and social enterprise (VCSE) sectors.
In July 2025, the Department of Health and Social Care published its Fit for the Future: 10-Year Health Plan for England, a wide-reaching roadmap for how the NHS should change over the next decade (DHSC, 2025). Whilst mental health strategies across England, Scotland, Wales and Northern Ireland share broad ambitions around prevention, recovery-focused practice, community-based support, reducing inequalities and the use of digital innovation to improve access, self-management and service delivery (Department of Health, 2021; Scottish Government, 2023; Welsh Government, 2025), the NHS England 10-Year Health Plan places particular emphasis on a shift from “analogue to digital” services and digitally enabled models of care and learning. The plan aims to shift more care out of hospitals and into local communities, embrace digital technology, and place greater focus on preventing illness before it starts. Recovery Colleges are well positioned to support these key shifts:
from “sickness to prevention”, both the primary prevention of ill health and the secondary prevention of reducing relapse, of minimising the impact on people’s lives and enabling them to cope;
from “hospital to community”, with care available in the neighbourhoods and communities in which people live; and
from “analogue to digital”, pioneering the use of new technologies in online learning, which is the focus of this briefing paper.
What do we mean by digital and online?
In this briefing paper, we consider digital and online offers at Recovery Colleges. While a few Recovery Colleges operate wholly online, most now offer digital or online options as part of their overall provision. ‘Online’ and ‘digital’ are sometimes used interchangeably, but they mean different things.
‘Online’ refers to aspects of the college that happen online, connected to the internet or other networks, for example, meetings on Zoom or Teams, social media, streaming or a live online form on a website.
‘Digital’ refers to digital aspects which a college may provide, whether or not these are online, for example, a registration form, workbook, video, audio file, or self-help material that can be downloaded, stored on a computer or smartphone, or burned to a CD, and read or completed offline.
Aspects of Recovery Colleges which may be digital, online or have a parallel online process include enrolment, evaluation, governance and leadership meetings, co-production and the provision of courses.
We do not discuss Artificial Intelligence in this paper, as it will be the subject of a future briefing paper, but we acknowledge that it is likely to have an impact on Recovery Colleges in the future.
Online and digital learning can take many forms, with its own benefits and limitations, as shown by some examples listed below:
Virtual online courses delivered in real time with trainers and fellow students using videoconferencing
Self-directed e-learning, often digital and sometimes online through a website, but could be emailed or downloaded, e.g. self-help workbooks
Blended learning
where some sessions are face-to-face, combined with other live online sessions' ownloadable handouts or self-directed work, or
where shorter interactive online sessions are supplemented with opportunities for reading and self-directed learning
Hybrid learning, where some students join virtually, online, while others attend in person
Recovery Colleges’ experiences of transitioning to online learning
Prior to 2000, Recovery College education was rooted in shared physical spaces in which trainers and students engaged in collaborative, recovery-focused learning. The in-person environment was considered essential to the Recovery College ethos, fostering empowerment, inclusivity, and mutual learning. As McGregor et al. (2016) point out, these spaces allowed the knowledge and experiences of individuals to flourish:
'Creates a space where the knowledge and experience of the 'patient' can grow and be explicitly owned, where a demonstrable change in power relationships goes a long way to account for the remarkable consistency of positive results for Recovery Colleges across cultures.'
Few Recovery Colleges had a large online or digital presence before the pandemic, leaving teams with little time for systematic planning for online processes or course redesign. The urgency of maintaining contact with students and staff meant that adaptation was often reactive rather than strategic. During this time, many Recovery College staff members were redeployed to clinical roles, adding to the challenge of sustaining educational services.
The transition to online learning was complex and varied widely across Recovery Colleges. Teams faced significant disparities in organisational support, access to online platforms, and technological proficiency. A range of online platforms were used - some NHS Trusts used platforms like Zoom or GoToMeeting, while others mandated Microsoft Teams due to information governance concerns. This created inconsistencies in how easily courses could be designed and delivered. Additionally, many Recovery College staff initially lacked the digital skills to translate recovery-focused, strengths-based education into an online format.
Early in the pandemic, online Recovery College spaces often functioned as supportive forums, reflecting the impact of social isolation on students and staff alike. As teams adjusted, different online learning models emerged to meet diverse needs, and hybrid and blended learning became more common, particularly in acute care or rehabilitation settings. Self-directed content was made available on online platforms such as FutureLearn, along with expert-patient programs that provided self-directed digital content on mental health and physical conditions. Recovery Colleges had to consider whether using co-produced content was sufficient to uphold their values, and how to co-produce the rapid organisational change needed whilst maintaining active co-facilitation and co-learning.
'We have gone Digital so doing courses online, which I have found very stressful since I am a Technophobe. Recovery College is quite challenging. It is so different to how it used to be. It's more led from above, less democratic and we have less involvement in making decisions.' Peer Trainer, Sussex Recovery College
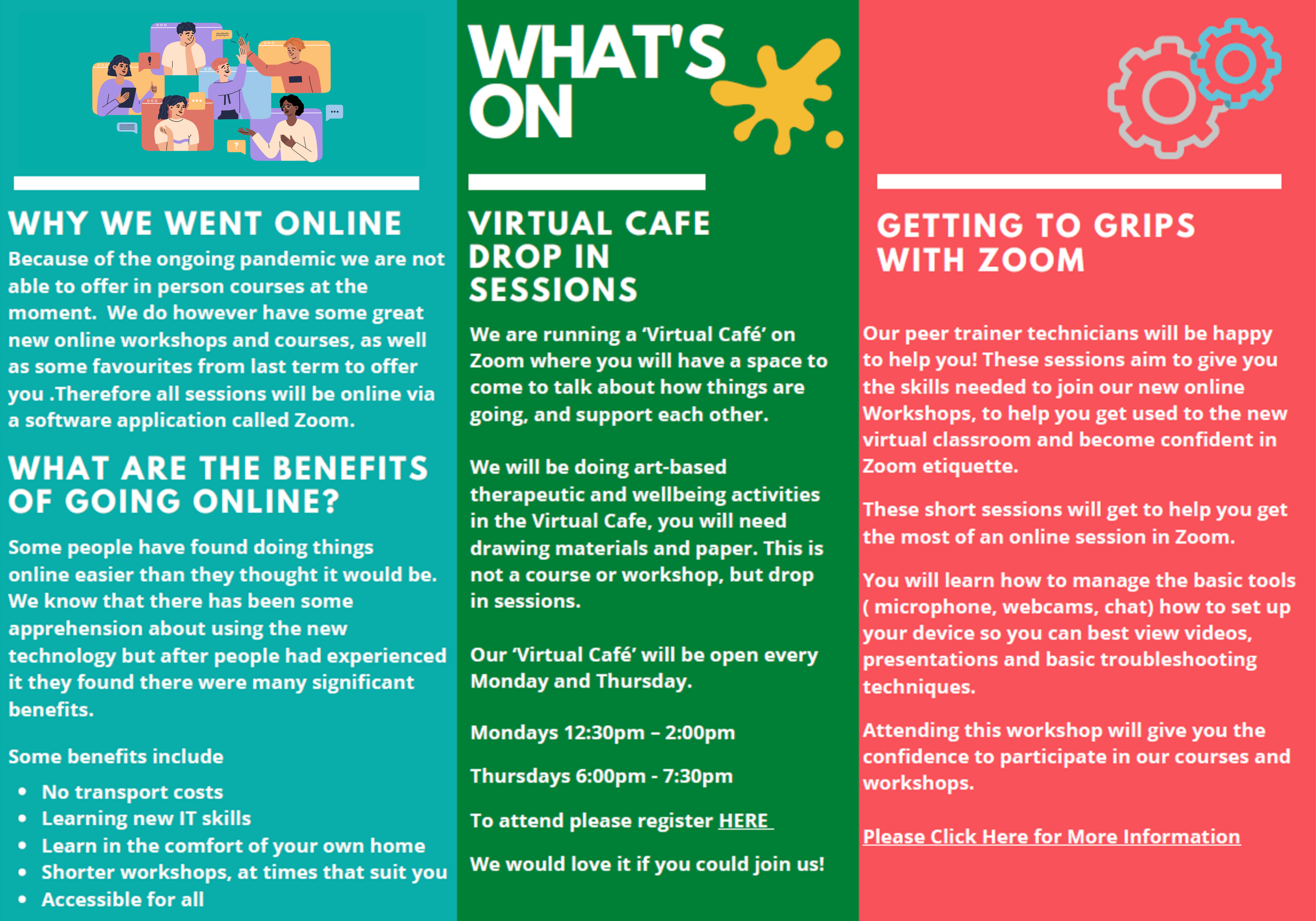
Sussex Recovery College held its first online courses in May 2020. They had already been developing online registration and feedback processes and held some meetings virtually. They were conscious of the impact of the Covid pandemic and changed ways of working for staff, students and the wider community. They facilitated a peer-led virtual café twice weekly to support the wellbeing of staff and students. They developed guidance for students and trainers on how to use GoToMeeting and then Zoom on mobile phones and overcome some of the differences in functionality between devices (Byrne et al., 2023).
Below is part of the prospectus when Sussex Recovery College went online during the Covid pandemic:

As Recovery College trainers gained confidence in online teaching and digital content creation, the essence of Recovery College education began to be replicated in some virtual spaces. Trainers learned to integrate presentation materials, facilitate discussions through Chat and Question and Answer (Q&A) functions, and create spaces for students to share their experiences and strengths. What initially felt like a loss of Recovery Colleges’ core identity gradually evolved into a new way of fostering recovery-oriented learning in a new space, proving that the values of collaboration, empowerment, and mutual growth could extend beyond the physical classroom. However, the transition to online learning presented both opportunities and challenges for Recovery Colleges. While for some it expanded access, encouraged collaboration, and introduced new learning methods, it also exposed issues of digital exclusion, resource limitations, and the importance of social connection. New ways needed to be found to ensure adult learning principles, co-production, co-learning and recovery orientation.
Blended learning approaches, with a mix of face to face and online learning, have helped students to engage in ways that work best for them, offering choice and flexibility. For example, when Dorset Recovery Education Centre (REC), in the
UK, could no longer deliver in-person courses, they developed a range of digital resources, enabling students to continue learning from home. Student feedback highlighted the benefits of this shift, and even after face-to-face courses resumed, the blended model remained popular, providing greater flexibility in how students engaged with recovery education. The key considerations, implementation processes, and experiences of moving online are explored in Case Example 1.
In the following sections, we outline some of the opportunities and challenges associated with digital and online offers at Recovery Colleges in terms of the key features:
Accessibility, inclusivity and being open to all
Adult learning (education) and online teaching skills
Co-production, co-facilitation and co-learning
Recovery oriented and strengths focused
Case Example 1: The Dorset Recovery Education Centre (REC)
Joanna Peckham (REC Co-ordinator) and Jane Carey (Peer Lead for Education)
The REC was established in March 2012 and is delivered as a partnership between Dorset HealthCare (DHC) and Dorset Mental Health Forum. The Covid pandemic was the starting place for the REC to consider how resources could be made available to people in their own homes. It also gave us the capacity to look at developing resources in line with our existing curriculum that students could access online. At this stage there were a few key areas for consideration such as:
Accessibility
Shared learning
Continuing co-production
Modelling recovery and the challenges faced
Offering opportunities to connect and share learning where possible
Endeavouring to make the offer inclusive and open to all. Reaching out to those who may face challenges in navigating their way through a changing service
Peer support and sharing amongst students
Feedback from those accessing the resources
Wellbeing of the staff team
Skills available in the team to translate, as far as possible, some of the essence of Recovery Education
We chose to develop webinars in two formats for registered students to attend, one platform would be anonymous with use of a chat box, the other would use cameras and microphones and be more like a virtual classroom. We developed podcasts and short video clips which were accessible to anyone. These were fairly time effective and quick to produce and have the capacity to be accessed at any time. We needed to consider the needs of students without access to the internet so workbooks were developed which could be sent out to students on paper. Key changes made to the REC operating process included:
Introduction of flexibility for enrolment appointments. These appointments can now take place over the phone or through the Attend Anywhere platform
Creation of learning resources for students; podcasts, video clips, workbooks
The launch of live webinars for students who are registered and enrolled
The launch of a new DHC REC Webpage and Social Media pages in an attempt to communicate our offer more widely
A new DHC webpage was launched within months to incorporate a ‘learn online’ tab and to break up some of the information and text on the webpage
Student experience was surveyed following the introduction of online learning, and we found that students were adopting a blended learning approach, using podcasts, videos, workbooks and accessing webinars. Following the reintroduction of face-to-face courses, this blended learning approach continues.
Increasing Access and Inclusion – Open to all?
Recovery Colleges have always sought to be inclusive and to work towards being genuinely open to all. They have tended to be more representative of local populations than other mental health services, for example, they may be more accessible to people who are often underserved and underrepresented in mainstream mental health services, such as people from LGBT groups and people from ethnic minorities (Meddings et al., 2019). However, funding, governance, and commissioning structures also play a part in accessibility. For instance, some NHS-operated Recovery Colleges are open to entire communities, while others prioritise people using mental health services, carers, and staff.
The shift to online learning enabled Recovery Colleges to reach a wider or different group of people, removing geographic and some logistical barriers and potentially making Recovery College education more inclusive. There can be increased accessibility due to reduced costs and increased course variety and flexibility.
This expanded reach enables them to contribute more effectively to public health and mental health promotion through recovery education, but at the same time, people with more serious mental health challenges, including people using secondary mental health services, may experience a reduced offer.
One of the main benefits of online learning is its ability to reach geographically distant individuals, such as those in rural areas or relatives who live in different places from the people they care about, and to accommodate those with demanding schedules, such as carers. Within Recovery College networks, managers reported that when courses went online during the Covid pandemic, more students attended who were not local, more men, more younger people and more staff with their own wellbeing issues. In Sussex, data shows that when more courses were online, the proportion of students who were carers or younger people increased (Sussex Recovery College, various years). More children and young people, and more people from primary care wellbeing services, attended the Digital Recovery College (Patmore, 2020). This may also have been because the courses on offer differed, because the shorter and single session courses during the pandemic may have suited these people more, or that these were groups with increased challenges during the pandemic, or groups that had greater access to IT. It may also have been that the difference was due to decreasing numbers of other students, fewer older people or fewer people with significant mental health challenges.
Groups that appear to have benefited from online learning include:
People who find face-to-face classes difficult, for example due to
geography, especially in rural areas
lack of accessible public transport to college locations
finding it more difficult to leave the house
challenges of being in social groups
Carers
People from some minority communities
Clinical staff
People who work full time
People with access to IT and who are conversant with virtual contact
Younger people
Middle class highly educated people
People with more mild mental health challenges
People under forensic mental health services
The transition to online learning also led to increased enrolment of students with diverse disabilities, including those who find travel or being in a face-to-face setting more difficult. For instance, those with visual impairments could use adaptive technologies, and neurodivergent students often felt more comfortable engaging online due to reduced social pressures. It allowed clinical staff to participate more easily, both in terms of their own wellbeing and integrating recovery-focused education into their professional development. Sometimes staff might feel more comfortable co-learning with people from a different area than where they work, and this is enabled through online courses. Online learning also reduces the time taken from their core role and offers opportunities to access learning outside of working hours.
People from some (but not all) diverse minority communities have benefitted from online options. Joining with others from different geographical areas enables large enough cohorts for bespoke courses to be created for that group, such as LGBTQ+ people or veterans. However, fewer people from ethnic minorities attended Recovery Colleges when they moved online during the pandemic, and there were issues
with digital exclusion and digital poverty, including people being unable to afford computer equipment and not having digital skills (McPhilbin et al., 2024).
Online Recovery College students also tend to be more highly educated, with many having attended university (Briand et al., 2024). Online delivery may be helpful for family supporters, but less accessible for people living with dementia as it is harder for tutors to actively facilitate their involvement. It may also risk digital exclusion for older people who are less affluent and able to afford technology, or less computer literate but increase inclusion for people who can’t travel to courses (Wolverson et al., 2024). Linda Birt and colleagues have been evaluating Recovery College support post-diagnosis of dementia:
‘We were able to compare online course delivery with face to face and single sessions with up to three sessions. We found online delivery was helpful for family supporters but less accessible for people living with dementia as it was harder for tutors to actively facilitate their involvement. While in-person single sessions had positive outcomes, the opportunities for development of confidence to be involved and social connections were most actively seen in courses that ran in-person over three sessions.’ (Linda Birt, researcher)
More people with milder mental health challenges, and fewer people with severe mental health challenges access Recovery Colleges through online registration, courses and materials. Where Recovery Colleges were once predominantly accessed by students involved with secondary care services, there has been a notable shift toward participation from students linked to primary care, public health, and mental health promotion services. The introduction of online Recovery College options has also enabled more people using forensic mental health services, who previously could not attend in-person courses to participate (McPhilbin et al., 2024).
Case example 2 illustrates how digital online Recovery College courses may widen access to people using forensic services.
Case Example 2: Reflections on an online Forensic Recovery College
Oliver Kane, Betsey Walker and Bev Howards, Forensic Recovery College and Education, Midlands Partnership NHS Foundation Trust
MPFT has been developing its Recovery College offer since 2024. Within the secure services division of the Trust, the value of providing access to Recovery College learning for inpatients was recognised early on, though practical barriers such as geography, transport and Ministry of Justice restrictions often limited meaningful access.
Since April 2024, we have re-established online and hybrid delivery within forensic services. Starting from the ground up has allowed us to design an approach that genuinely fits the secure environment rather than adapting a community model after the fact. This has enabled service users to access recovery education consistently, while also connecting them with colleagues, lived experience practitioners and partners beyond their immediate ward or site.
As we move through 2026, the Forensic Recovery College now facilitates a live prospectus for both service users and staff and is supported by multiple Experts by Experience working across a range of recovery and involvement workstreams. Service users are no longer engaging in isolated activity, but contributing across courses, lived experience sessions, co-production forums and involvement groups. This creates continuity, progression and a clearer recovery pathway.
Currently, service users across low and medium secure settings are engaging in full length recovery and wellbeing courses, many for the first time. Feedback and observation show increased confidence, skill development and greater participation in everyday ward life. Learning is increasingly being translated into communication, self-advocacy and peer support.
Challenges remain. Digital access can be inconsistent and online delivery cannot fully replicate the relational depth of in person work. Facilitators continue to adapt sessions carefully to ensure safety, engagement and accessibility, while navigating technical issues such as connectivity, audio and platform limitations.
Despite this, online and hybrid delivery is now a permanent and valued part of our model. It has extended reach, amplified secure service user voices, supported multiple recovery workstreams, and strengthened a culture of involvement and co production across forensic services.
Digital exclusion is a significant issue for online Recovery College offers. Many students face barriers to participation due to a lack of technology or confidence in using digital platforms. Students report that the enrolment process and accessibility are important contextual factors; therefore, it is as important to make online enrolment and introduction accessible as it is the courses themselves. Not everyone has access to computers or the necessary technology or feels confident using it. Barriers may be at the stage of registration if this is wholly online, when attending courses or in being heard in research and course feedback processes. Some Recovery Colleges have taken responsibility for supporting digital access by providing technical support and offering alternative learning formats. However, digital poverty and a lack of digital skills remain ongoing challenges. Supporting individuals to access online and digital content has become a crucial aspect of Recovery Colleges’ roles, ensuring that learning opportunities extend beyond course content to include digital skills.
‘It may be important to offer both online and face to face options. Some students find it convenient to register online, whereas others find it challenging. I recently helped someone face to face to register with the Recovery College. They had come to the open day to enrol as they struggled with reading and with IT and were daunted by the online process. They gained confidence talking to someone in person.’ (Clinician Trainer, Sussex Recovery College)
Online learning can be a stepping stone, allowing students to engage from the safety of their homes before transitioning to in-person sessions. It enables students to develop an understanding of what Recovery Colleges look and feel like before attending in person. Online sessions may be shorter, providing a gradual transition into classroom settings. This step-by-step approach can help students build confidence and familiarity with the learning environment. Additionally, virtual platforms can allow for more options in terms of individual learning plans, enabling teams to create tailored study paths for students who may otherwise struggle to engage in face-to-face settings.
An example of this approach is ‘Recovery College Online’, which, during the pandemic, decided to open access globally. This initiative has continued beyond the pandemic, expanding the reach of recovery education and fostering an inclusive, international learning community, which is described in Case Example 3.
In response to these ongoing challenges, Recovery Colleges have supported students to overcome barriers to digital and online learning, recognising that access to technology and digital skills is now integral to participation. By offering tailored assistance and flexible learning options, they strive to ensure that everyone has the opportunity to engage with recovery education, whether online or in person. This commitment to inclusivity broadens access and helps people build confidence and digital competence alongside their personal recovery journeys.
Case Example 3: Recovery College Online
Joanne King (Recovery College Online Operations Manager)
Recovery College Online (RCO) was first developed in response to the success of ARCH Recovery College, Durham. ARCH Recovery College is only available for people using services living in County Durham, but due to its success, Tees, Esk and Wear Valleys NHS Foundation Trust (TEWV) wanted to replicate this with something that would be available across the whole of the organisation, and eventually, across the world. This is when Recovery College Online was developed, with the launch in March 2017.
Whilst we initially adapted the courses used at ARCH to create an online version, we have since gone on to create around 80 self-directed online courses, with over 70 currently live. All courses are free to access with the creation of an online account and can be completed by anyone, anywhere in the world. RCO was originally for people living within the geographical area covered by TEWV, however during the Covid-19 pandemic, a decision was made to open access globally, which has remained since. Our information is applicable to all, as the information we provide, including our E-Learning, is non-Trust specific.
Our trainers often have their own personal experience of mental health problems and using mental health services, often with teaching or training experience, as well as a strong understanding and knowledge of what recovery means. Once in post, they are fully trained in using the software and programmes we use for course creation, with continued support and training. They work closely with professionals and involvement peers (volunteers with lived experience) to ensure that all our courses and content are entirely co-produced.
Students are expected to have a general understanding of online courses and distance learning, as well as basic computer literacy. We offer support in terms of account login issues, accessing certificates, choosing courses, and signposting to relevant services and support, or recovery colleges local to the student. The E-Learning is not delivered live via Zoom or MS Teams, rather is it uploaded to the site to be available 24/7 and can be revisited as many times as a person wishes.
We include our ‘Terms and Conditions’ and ‘House Rules’ in the course information for each new registered student to view. We encourage self-reflection throughout our courses with the use of ‘consider more’ sections, with reflective questions and areas of thought, to encourage progression, recovery, and strengths-focus.
Adult Learning (Education) and Online Teaching Skills: The Need for Developing New Skills
Facilitating online sessions requires different skills and approaches from face-to-face teaching. Trainers need to adapt to digital learning environments while maintaining the Recovery College ethos of recovery, empowerment and shared learning. New technologies demand:
Training in online facilitation
Access to appropriate equipment
Support for students unfamiliar with digital tools
Additional funding for software and resources
‘It’s different teaching online – you have to think carefully about how to manage the session and ensure there are different types of activities and that everyone is included and that it is paced in a way that works for everyone. As a trainer I find it harder to keep an eye on how everyone is doing or to help people who may find an activity more challenging.’ (Clinician Trainer, SLaM)
Richardson (2026) identifies three elements to successful online teaching:
Connection: creating a sense of belonging to the group and the learning itself and to facilitating co-learning. Connected students are more likely to attend, study and be successful
Content: active learning and structured sessions, activities that are tailored to online delivery and include a mix of active learning activities whereby students are more actively engaged rather than passively receiving information from a teacher, using break out rooms, discussion and possibilities for interaction and physical movement
Cohesion: creating a virtual learning environment and using technology in a way that is clearly organised, user-friendly and consistent across courses, and where resources are appropriate and accessible for all students
It can be helpful to build connection among students by enabling them to congregate and get to know one another, for example, enabling early entry into the virtual classroom for more informal chat. As in face-to-face teaching, facilitators might take time and support to learn how to interpret silence and determine whether it is due to thinking time or apathy, and it is useful to have activities for students when there are gaps. Establishing ways in which tutors can see if students might require extra support, for example, picking up on non-verbal cues, or if the student becomes distressed, is an important way of creating a safe learning environment for both students and tutors. These processes may take time to establish as a team. In a physical setting we can discretely check in with them and do this; online environments require new strategies to ensure all participants feel supported.
Developing the skills to manage online spaces, and in hybrid courses to do this whilst also managing the in-person classroom takes time, training and support. The added complexity of hybrid facilitation may require an additional co-facilitator whose role is specifically to manage the online platform, whilst the co-facilitators manage both spaces and to ensure online students are included equally to in person ones. It takes a great deal of skill and care to follow both the verbal and non-verbal communication in the in-person room and also the verbal, visual and chat communication in the online space. Trainers may benefit from having two screens so that they can see slides or notes and also see their co-facilitators and all the students in the class.
Different learning experiences may be favoured in online spaces. For example, students are more able to search on the internet or share resources as part of an online class. Some, but not all, online platforms are able to replicate flip charts, screen sharing presentations and breaking out into smaller groups. Social media platforms, chat forums and podcasts may be used to share information, engage students and foster community, especially among younger learners and carers. The chat function in online courses may feel more comfortable for some students who are not confident speaking out in class, whereas others might prefer to make eye contact and speak one-to-one to a trainer in person during a break. Some students also find it helpful to have the slides emailed to them:
‘It was helpful to be emailed the slides of the sessions, so I could refresh my memory and print off what I needed at home.’ (Student, Sussex Recovery College)
Some skills or courses are better taught online, whilst others may be better face to face. Practical skills requiring physical or tactile practice may be less suited to online or distance learning whereas online learning may be more helpful for auditory or visual training with the use of videos or simulations or as supplementary to face to face teaching (Abassi et al., 2020; O’Brien and Forde, 2023).
Privacy concerns, group dynamics, and ensuring safe, inclusive learning spaces add complexity. Establishing clear guidelines around online platforms helps to protect students’ privacy and maintain confidentiality, especially in group settings. Some Recovery Colleges, for example, require cameras to be on during sessions, while others make this optional to respect personal preferences, and encourage people to use a photo if they feel unable to have their camera on. In an online classroom we can only see what is on the screen and not, for example, an abusive partner in the room next door, the lower half of a person or an additional person in the room, perhaps a child or another adult who is observing. This can raise potential confidentiality and safeguarding issues. Safeguarding protocols and training need to consider the different potential risks arising online and include how to keep people safe and minimise risk and how to identify and respond to any issues if they do arise. To ensure a safe and supportive learning environment, learning agreements on issues such as camera use, raising hands to speak, breakout room protocols, and chat functions can be collaboratively developed and agreed upon by each group of learners and facilitators.
Online Recovery College Learning Agreement
We will agree to the breaks
You can always use the chat
Be mindful of your environment and other people hearing or accessing the confidential space
Please ask permission before recording the session
The shift to online learning prompts Recovery Colleges to rethink their approach, balancing the benefits of digital and online education with the challenges of accessibility and resources and maintaining a strong sense of community. South London and Maudsley NHS Foundation Trust demonstrate this adaptation in Case Example 4, which details how their Recovery College team navigated the transition to developing new skills.
Co-production, Co-facilitation and Co-learning
A key consideration for digital online learning in Recovery Colleges is how these approaches and self-directed learning models align with the co-produced ethos. Co-production is about ‘doing with’ people rather than ‘for’ people and valuing different kinds of expertise (lived and subject matter expertise; co-facilitators and co-learners) equally. Co-production is not a ‘one off’ exercise but an iterative process of review and re-creation that involves not only the tutors but also those attending the courses. It happens at every level of a Recovery College, including the co-production of courses and college systems, and co-production and co-learning within the online classroom itself.
There is anecdotal evidence that people find it harder to coproduce online. Members of the Imroc Recovery College Learning Set expressed that their greatest fear about going online with the Recovery College was that co-production wouldn’t be done properly if it were not face to face.
‘When co-producing the material, if you are not in the room, you are not seeing the body language and there is a barrier to the trust you need for sharing and co-producing.’ (Peer Trainer, SLaM)
Case Example 4: South London and Maudsley NHS Foundation Trust (SLaM)
Kirsty Giles (Recovery College Manager) & Mark Dalgarno (Deputy Manager)
In South London and Maudsley NHS Foundation Trust (SLaM), we moved from classroom training to online at the start of the Covid-19 pandemic. As this was an unforeseen circumstance it resulted in the RC Team having to learn as we went along, but in the true nature of co-production this was in a collaborative and supportive way. Some members of the team were more experienced in technology and taught the other staff how to use both webinars and MS Teams, ensuring our students did not miss out on their learning. In the beginning,
we had more experienced/confident members of our team oversee/provide additional support to each course to make sure the technology worked, they set up and read out comments from the students and contributed to the training, helping build the confidence of the other trainers.
We adapted our courses that were previously co-produced and co-delivered, creating both webinars and MS Team workshops. As well as this, we co-produced new courses that continue to be delivered online and in-person. The courses and workshops followed a similar format from before, and we ensured co-learning via the chat function within the webinars, reading out the students’ comments, questions and answers. In MS Teams, we made use of the wide group discussion and break-out rooms to allow students to feel connected and included.
In SLaM Recovery College we have external course providers from the SLaM and other specialist areas. They were able to continue to provide training, with our Peer Trainers and moderators supporting them to use the technology. The move to online learning has provided us with the opportunity to open our doors to many and engage with a wider community.
In SLaM Recovery College, one of our Peer Trainers is an IT champion and provided training for members of staff as well as students, alongside the digital support team. This was cascaded throughout the team, and as each person learned how to use the technology they taught each other and external trainers. As a whole team, we learned how to use accessplanit, a student learning system, with training from the service provider and a Peer Trainer taking on the lead role and offering continuous training for the team.
We realised that several students, who may find it difficult to attend face to face workshops, preferred to attend online. Webinars allowed for anonymity and a different method of teaching, and MS Teams provided a virtual connection. As a result, we continue to offer online training open to all, in conjunction with the classroom training which is open to those connected with SLaM.
‘Trying to coproduce online only causes difficulties, you can be isolated, not work so dynamically, not be able to bounce ideas around in the room. I think you need at least some in-person meetings.’
(Peer Trainer, CNWL)
It may be that a hybrid approach to co-production could work best, whereby co-facilitators initially meet face to face to begin planning a course, but carry out preparation work separately, and then meet online to finalise the course and try out the planned online activities. It may also be that a course might be co-produced in person but then co-facilitated online. Again, Recovery College Academic Boards and other forums might sometimes meet face to face but have virtual online meetings in between.
For self-directed learning, the digital materials can be co-produced and include content to help people feel they are ‘not the only one’, and then students access chat forums or other platforms to enable co-learning and peer support. During online teaching sessions, co-trainers need to find new ways of communicating with each other in order to co-facilitate and compensate for the lack of in-person cues. In a physical classroom trainers get to know one another and can pick up on minor changes in body language, tone or mood. In online settings we need to find new ways to communicate with each other about the process, how the session is going and whether anything might need to be adapted. Some trainers have a second device, such as a phone, where they can message each other about how their teaching is going and any changes to the plan.
‘The dynamics between trainers, trainers and learners and between learners are different when you are not in a physical space. You make assumptions and can’t see their height, can’t smell them, you don’t know who they are, can’t pick up so well on non-verbal communication. People are more reserved and you don’t get the same cohesion as a group. There is not so much trust in the online space.’
(RC Manager, SLaM)
Co-production brings together different types of expertise. When delivering online content in Recovery Colleges, this may also include expertise in IT, digital and online skills. When co-facilitating a course there may be three co-facilitators: a peer, a subject matter expert and someone (who may also be a peer or subject matter expert) who takes responsibility for IT and digital expertise. This third co-facilitator might support students or trainers if they have IT issues, support facilitators with visual and audio, manage the chat function, screen sharing and breakout spaces so that everyone has the opportunity to participate. A third facilitator may also step in if one of the co-facilitators’ internet connection is lost, ensuring continuing so that the course may continue.
In relation to co-learning, students who attend Recovery Colleges online continue to appreciate the testimonies of other participants, to learn with people from different backgrounds and benefit from the richness of their expertise (Briand et al., 2023). There seems to be evidence of co-learning between students from diverse backgrounds (e.g., education and health care providers, university students, people in vulnerable situations, family/peer caregivers, workers, managers, retirees/seniors, citizens) as well as distinct trajectories of change depending on background (Briand et al., 2024; Rapisarda et al., 2025).
‘I would describe it as a type of collaborative learning. Making sense of multiple points of view, putting them together, and advancing the process of reflection and reasoning. I really think there is a co-construction happening.’
(Student, CASR-HRLC)
However, some people feel that in online classrooms co-learning can become diluted and it is harder still to replicate in a podcast or self-directed learning.
‘You lose the impact of co-learning, of having carers, peers, staff and service users in the same place co-creating the experience and answers to questions.’
(Clinician Trainer, Sussex Recovery College)
Much co-learning happens to one side of the classroom agenda itself, and the opportunities to develop links with other students may be seen more in longer in-person courses. Within the classroom, approaches discussed earlier may help greater co-learning, for example use of breakout rooms for small groups and pair work and encouraging people to mix more with one another. Use of chat forums and seeing comments of other students when engaging in self-directed learning can begin to offer a taste of the co-learning experience. With more staff and carers accessing online Recovery College courses there may be more or different opportunities for co-learning. We need to consider how different people learn and function in groups and find reasonable adjustments and different ways to support students.
‘The sharing of examples and ideas from everyone including the trainers.’
(SLaM Recovery College service user student on impact of isolation course)
Broader aspects of online co-production may include using online or digital surveys of students and/or trainers (peers and subject matter experts) in order to learn what’s gone well or could be improved, and how to continue co-producing courses and improve the quality of the Recovery College online offer.
Recovery oriented and strengths focused
Recovery Colleges reflect recovery principles in all aspects of their culture and operation. They are strengths focused and offer hope, control, opportunity and connectedness, and this should be no different when learning is online. Digital and online Recovery College courses are likely to be recovery focused in their content. They also need to be recovery focused in the way they are facilitated and to offer an online environment that conveys messages of hope, possibility and empowerment. Care needs to be taken to use platforms where the online environments can enable this, and where trainers can set up their own backgrounds with pictures and writing that give such messages. They might include artwork, books, plants or certificates of achievement. Lessons plans might include opportunities for students and trainers to demonstrate their skills and strengths.
Students at CASR’s online courses report feeling connected, collaboration and equality:
‘Respectful. Everyone listened. It was quite amusing because we didn’t know each other; it was brief sequences, but we sensed each other’s desire to support one another. It was quite amazing because even if we didn’t know each other and we saw each other only for 6 hours, there was something, there was a bond.’
(Student, CASR-HRLC)
At SLaM Recovery College, student feedback showed that 70-80% students felt more hopeful after attending an online Recovery College course, but only 40-50% felt more connected, although there was also variation between courses. Differences may have been associated with topics, activities, tutors, the mix of co-learners or the length of courses.
‘This session was very valuable, and I enjoyed the learning and sharing. I’m pleased to take part in it and take my learning from it. The best thing about it was the wellbeing wheel which made me feel part of the whole picture.’ (SLaM Student staff member on Introduction to Recovery Course)
‘People who already felt marginalised or were lonely told us that they preferred face to face courses and did not like the online self-management courses’
(SLaM Practitioner Trainer)
Without in-person interactions, innovative solutions are needed to enable students’ sense of connectedness and to preserve the community-focused ethos of Recovery Colleges. They need to find ways to foster peer support and connections between students. This could enable new opportunities for social connection, for example, for people in hospital or who are housebound, or for people to link with others in a minority community.
Ensuring emotional safety within the classroom is a key element of recovery focused learning. Some ways that might support this include:
Having enough facilitators available to moderate discussions, oversee breakout rooms, and manage chat functions so that students connect with one another and the material
Co-producing group learning agreements which take into account the strengths, needs, hopes and preferences of each group of learners
Making time for students to connect informally before and after sessions by opening them 10 minutes early and leaving them beyond the session’s end time. Shared break times can also encourage connection
Encouraging students to exchange contact details and arrange meet ups where this feels appropriate
Offering dedicated social sessions, informal virtual meetups, structured peer networking opportunities, and integrated discussion forums.
Creating opportunities to support students to gradually access face-to-face opportunities where possible, so that the transition from online to face to face learning feels supportive
It can also be a challenge attending face-to-face learning, as noted by a student who had first attended online during the pandemic:
‘It’s a challenge moving back to face-to-face’
(Student, CNWL Recovery College)
By offering courses both online and in person it may be that Recovery Colleges can build on the strengths of students and offer more choice, for example, as we have discussed earlier, enabling someone who is housebound to attend a course when they wouldn’t have been able to do so in person. For some an online course may be the best opportunity for accessing a Recovery College course and connecting with other people, the college and its values. It may be that online courses are a way of belonging, being accepted and included. It could be a stepping stone or gateway to greater involvement.
Case Example 5 illustrates a student’s experience of accessing online Recovery College courses.
Case Example 5: Student Experience
My experience of being an online student at Thurrock Recovery College.
I have been with the Thurrock Recovery College for very, many years, it might be ‘only now’ that I have appreciated that Recovery is an on-going process; things don’t ‘magically change’ and that I have to put the work in too.
I think that sometimes putting the work in is a lot for an individual and have come to realise it’s ‘day-in-day out’ and also has to come from the person, ie me/myself to try to make changes which, especially on a bad day when things can be a real struggle and challenge, is not easy.
The Recovery College has provided a safe space online and I value the techniques and ideas that come from them and it is very much ‘do what works for you’ and they suggest very many things to take away and utilise to try and cope. I have appreciated all of the courses that I have attended as I aim/try to get something from everything I do. The peer support help on the courses gives a nice feel and tutors join in with scoring themselves/ourselves from 1-10 on some of the courses I have been on and so the feel is nice as though everyone else is only human too and it helps to hear the tutors and other people’s short stories and their experiences sometimes.
I particularly like the Zoom courses as they tend to keep me focused on myself and listening, they are so easy to set up and I can do from the comfort of my own home. I always look forward to seeing the new timetables and I have really gained things by being on the Zoom courses with the trainers and others. I genuinely look forward to attending the courses provided.
I thank the Recovery College for the work they do and support that is given so much so that I am hoping to find a voluntary position leading to part-time work within organisations such as this.
Increasing Need for Resources and Organisational Support
Organisational support is necessary in order to deliver high-quality, accessible online learning. Maintaining an effective online learning presence requires sustained organisational backing, technical infrastructure, and dedicated resources. Content creation, platform maintenance, and technical troubleshooting demands continuous investment. For Recovery College staff, this means training in online co-facilitation and teaching methods, and time for content development, alongside the need to build new digital skills (Vallarino et al., 2026).
Developing digital learning tools, such as podcasts, e-learning packages, and webinars, requires dedicated staff time and funding for equipment and software. Technical problems, delayed audio and students unintentionally interrupting can deter students from future contribution and make facilitators more uncomfortable sharing their lived experience (Merly McPhilbin et al., 2024).
‘It takes time—it’s not possible to do the online work as an add-on and do both effectively.’
(Peer Trainer, CNWL)
Enhancing Collaboration Across Recovery Colleges
By removing physical constraints, Recovery Colleges with an online offer can expand their reach beyond local populations, moving toward nationwide and international recovery education. The International Recovery College Community of Practice has long supported international collaboration and learning between Recovery Colleges. Imroc also facilitate an online Recovery College Learning Set with colleges from different countries. The ability to connect and collaborate across the United Kingdom (UK) and internationally, through various platforms, can strengthen the Recovery College community. It allows students and staff from different Recovery Colleges to collaborate more easily, encouraging shared learning, shared course delivery and joint initiatives. For example, “Help for Heroes” facilitated collaboration between multiple Recovery Colleges, broadening access and pooling resources and developed a train the trainer resource that enabled different Recovery Colleges to develop courses for veterans.
Promising findings for Online and Digital Recovery College offers
Emerging evidence suggests that online Recovery College offers can deliver a range of benefits for learners consistent with the overall Recovery College research. After attending a Recovery College online, students have improved knowledge and skills, self-management strategies, improved wellbeing, empowerment and connection with others, and possibly reduced prejudice, stigma and self-stigma (Briand et al., 2023, 2024; Rapisarda et al. 2022). However, it is possible that the level of improvement may be less than for those attending face to face courses, with less long lasting or significant improvements. This could be due to the online nature itself or due to other factors, such as courses tending to be shorter and attracting a wider range of people with less severe mental health challenges (Rapisarda et al., 2022).
Students who choose to attend online courses have a positive experience, similar to that of students who choose face to face courses, with high levels of satisfaction (Rapisarda et al., 2022) and 96-100% say they would recommend the online course or college to others (Sussex Recovery College, 2022 & 2021). They also give similar feedback, for example, about the quality of the learning environment and connecting with others who share similar experiences:
‘It was very informative and pitched at a level everyone could understand’; about connection and co-learning ‘connecting with others about similar struggles.’ (Student, Sussex Recovery College)
‘I have never attended an online workshop like this and found it both helpful and comforting.’ (Student, Sussex Recovery College)
‘I learnt stuff I didn’t know before that I hope will be helpful for me moving forwards and made me feel open to joining further sessions / courses at Recovery College’. (Student, Sussex Recovery College)
Nonetheless, online formats may not suit everyone:
‘I find online meetings quite hard work due to sensory issues and concentrating over multiple screens. I do prefer face to face environments, however, do also understand the constraints which mean online meetings are sometimes necessary.’ (Student, Sussex Recovery College)
The mechanisms of action at online Recovery College courses, or the reasons why they work, may be similar to those in other Recovery Colleges. Students describe a context of recovery values, an inclusive learning space, equality, co-constructed knowledge and mutual support (Sauvageau, Bellemare and Briand, 2025). This is consistent with the previous findings of Toney et al. (2018) and Thompson et al. (2021) who proposed that recovery ethos, equality, co-production and learning led positive outcomes.
Case example 6 describes the experience of the Health and Recovery Learning Centre in Quebec, Canada, an online Recovery College. They summarise their research findings as: “…online short-format RC training courses can slow the progression of psychological distress and prevent the deterioration of mental health and the aggravation of mental disorders in the general population and at-risk groups” (Briand et al., 2024).
Case Example 6: The experience of the Centre d’apprentissage santé et rétablissement - CASR (Health and Recovery Learning Centre - HRLC, Quebec, Canada): the effectiveness of a completely online Recovery college
Catherine Briand, Martine Vallarino, Filippo Rapisarda and Myreille Bédard
A Recovery College goes entirely online
In fall 2020, during the Covid-19 pandemic, the Health and Recovery Learning Center (HRLC), using the Recovery College model, adapted in-person courses to an online format. The HRLC team and its trainers were trained in techno-pedagogies to support the active participation of learners reaching people all over Quebec and beyond. Courses were promoted and offered to partner organizations and to the general population, upon an online free registration. Partner organizations represented the desired diversity of learners to ensure complementarity of knowledge as well as to reach groups at risk of mental health deterioration during Covid-19. Complementarity of knowledge implies the participation of people with diverse and complementary backgrounds (experiential, clinical, theoretical) in a collaborative co-production process, in which each person’s contributions are equally recognized and valued.
Over 1,000 diverse learners in two years
Since fall 2020, HRLC offered over 200 online courses lasting 6 hours (three 2-hour weekly sessions) to nearly 4,000 different learners. Courses were in real time, using the Zoom group meeting platform, and were led by two trainers working in dyad. The target audience included 12-18 diverse learners per course (health and education practitioners, managers, people in recovery, relatives, students, citizens). Learners were mostly women (84%), with an average age of 44 (21-79) and a high level of education. Three quarters had experiential knowledge, half had clinical knowledge, and 40% had received mental health services in the past six months.
Research findings confirm the relevance of online Recovery Colleges Research led by Prof. Briand evaluated HRLC’s activities. For a sample of 315 learners (representative of the diversity within the target audience), we compared people’s scores on a range of measures at registration, just after attending an RC course, and three months later. Results showed statistically significant immediate post-course improvements in anxiety, self-esteem/self-efficacy, and disclosure/ help-seeking behaviors. Improvements in well-being, resilience and optimism/ control over the future were also confirmed at the follow up, three months later (Briand et al., 2024).
Moreover, a previous qualitative study of online interviews with a representative sample of learners (n=14) also found positive outcomes (Briand et al., 2023) . Five themes emerged from the thematic analysis. After a RC course, learners mentioned: (1) updating and validating their mental health knowledge, (2) taking better care of themselves and their mental health (managing stress better and feeling more resilient and confident), (3) improving and modifying their behaviours and professional practices (in particular, reflecting on how to deal with their prejudices and stigma), (4) changing how they look at themselves and others (becoming more aware of oneself and others), and (5) interacting and connecting with others.
Quality and fidelity of the Recovery College
Understanding and reproducing the online Recovery College model’s key active ingredients are essential for achieving the desired outcomes. Establishing an egalitarian learning space is fundamental to the model’s effectiveness. Despite the online adaptation, the HRLC team rigorously followed RC principles. Trainers received over 30 hours of basic training (Train-the-Trainer Program), over 15 hours of additional online adaptation training, and regularly attended community of practice meetings (Vallarino et al., 2026). The diversity of learners and trainers ensured a mix of theoretical, clinical, and experiential knowledge. This enabled exchange between practitioners and people/relatives living with mental health problems in a safe place of mutual recognition free from judgment. Such interactions allowed for co-constructing an integrated knowledge within a transformative learning environment. To support trainers’ self-reflection and continuous learning, capacity-building tools have been developed to help them improve their competencies: a Trainer’s Guidebook, Course Co-Production Template, Self-Appraisal of Competencies, and Self-Observation of RC Key Ingredients (Vallarino et al., 2026). These tools help trainers to refine their skills and, identify tensions and leverage actions to ensure fidelity with the RC model.
Future perspectives: capacity-building tools to ensure model quality Findings support the potential for short, effective co-produced mental health education interventions to empower individuals and address psychological distress. Short online RC courses can be an effective strategy for supporting self-regulation and empowerment in general population and at-risk groups. Trainer support tools are essential for achieving these outcomes.
To join the Health and Recovery Learning Center (HRLC) in Quebec (Canada) – Centre d’apprentissage santé et rétablissement (CASR) du Québec (Canada) https://santeretablissement.com/casr.cemtl@ssss.gouv.qc.ca
Summary of challenges and opportunities of Recovery Colleges going online
Challenges
Opportunities
Digital exclusion:
Limited access to technology and a lack of digital skills may prevent some students from participating, including people from ethnic minorities, those with fewer financial and educational privileges, and individuals facing more severe mental health challenges.
Expanded access:
Reaches people who might otherwise be under-represented at Recovery Colleges, such as carers, staff, people in rural locations, those with milder challenges, and individuals unable to attend in person due to mobility or health issues.
Loss of social connection:
Reduced informal interactions can make it harder to build relationships and foster peer support and co-learning.
Increased diversity:
Engages participants from minority communities, including neurodivergent learners, LGBTQ+ students, and veterans, supporting inclusive spaces where people with shared experiences can connect.
Maintaining group engagement:
Online environments can make active participation and group discussions more challenging, potentially impacting overall engagement.
Flexible learning:
Enables self-paced study, access to recorded sessions, and varied formats to suit different needs, allowing individuals to participate at times that work best for them, including evenings and weekends.
Privacy and safety concerns:
Ensuring safe and inclusive online spaces requires clear guidelines and active moderation to protect all participants.
Wider geographical collaboration:
Strengthens connections between Recovery Colleges, facilitating shared courses and joint initiatives across different locations.
Resource and staffing limitations:
Developing digital learning platforms necessitates investment in infrastructure, staff training, and ongoing support.
Hybrid learning possibilities:
Blended approaches allow students to engage in ways that work best for them, offering more choice and flexibility.
Difficult transition back to in-person:
Some students may struggle with returning to face-to-face learning after becoming accustomed to online formats.
Stepping stone into in-person learning:
Online courses can help students build confidence and act as a bridge before attending face-to-face sessions.
Co-production and co-facilitation:
Require additional skills and thoughtful planning to be effective in a digital environment.
Empowerment and self-management:
Online delivery encourages individuals to take greater control of their well-being, fostering self-management and preventive care as highlighted in the context of the NHS's vision for community-based support.
Digital and Online Recovery Colleges as a service fit for the future
Recovery Colleges, and those colleges with an online learning offer for students in particular, are uniquely positioned to support the transitions outlined in the government’s Fit for the Future: 10 Year Health Plan for England (DHSC, 2025). Their integrated and flexible approach aligns with the NHS vision for modern, community-centred, and digitally enabled health and social care, empowering individuals to take control of their wellbeing.
From hospital to community
Recovery Colleges extend well beyond traditional clinical settings. Digital Recovery College platforms can act as a bridge between hospital, other health and voluntary sector services and the community, making recovery resources and educational opportunities accessible to people wherever they are, whether early in their wellbeing journey on hospital wards, in forensic environments, or living in the wider community. As one Recovery College manager (SLaM) described:
‘You can beam RC into the wards... and enable people in forensic to access it. This highlights the flexibility and inclusivity of digital delivery.’ (Recovery College Manager, SLaM).
The expansion of Recovery Colleges into the digital sphere can support the development of community-based care hubs as outlined in the 10 year health plan. By embedding Recovery Colleges within these hubs, recovery-focused educational programmes can become seamlessly linked with a broader network of health, social care, and voluntary sector services in local communities. This integration positions Recovery Colleges as a central access point, where people can find tailored recovery resources alongside easy pathways to additional support, addressing a wide range of needs.
Where online, Recovery Colleges can offer increased accessibility for some, allowing people to engage with recovery and wellbeing courses and other online materials closer to home and at times that suit them, including evenings and weekends.
It directly supports the plan’s ambition for care to happen as “locally as it can”. Ultimately, this integrated approach strengthens preventative care, encourages self-management, and empowers individuals to take control of their wellbeing, fully aligning with the NHS vision for modern, community-centred health and social care.
‘It expands personalised care options closer to where people live – digital Recovery College allows people to choose what would be most helpful to them …another venue or spoke where the college holds courses.’ (Recovery College Manager, SLaM)
Additionally, Recovery Colleges’ digital and online offers can create inclusive spaces where minority groups and people with shared experiences can connect and support one another, finding their own community. They enable the formation of peer groups that foster mutual support and a sense of community, for example, LGBTQ+ people facing health challenges such as diabetes, or veterans managing trauma, connecting with one another, no matter where they are based.
From Treatment to Prevention
Digital Recovery Colleges support the shift from treatment to prevention by widening access at every stage of the recovery journey, ensuring that support and education extend well beyond traditional clinical settings. As one manager explains:
‘It gives us the opportunity to open up our curriculum to the wider community.’ (Recovery College Manager, SLaM)
With their digital platforms, Recovery Colleges enable anyone to participate and learn about their own health and wellbeing, and how to live well with them, regardless of where they are in their recovery. With open access, general practitioners can signpost people to Recovery Colleges. People can choose to enrol online, download resources and take a course supporting them with tools to stay health, accessing early intervention support and with self-management skills. This supports the NHS’s aim for proactive, preventative care, empowering people to take control of their health and wellbeing before issues escalate.
‘Our online programme means we can invite the community in; anyone can attend, and it inherently has a health promotion, health prevention element.’ (Recovery College manager, SLaM)
Recovery Colleges can also support secondary prevention for those already living with mental health and other long-term conditions. People who enrol with Recovery Colleges are better equipped to manage their health, resulting in reduced relapse rates and fewer hospital admissions; they have improved wellbeing and quality of life and are more likely to be in work or education (Bourne et al., 2018, Perkins et al., 2018; Ronaldson et al., 2026 pre-print). Although most research has focused on in person courses, some students in the above studies have registered or obtained materials online or digitally. The Canadian research discussed above highlights the positive outcomes associated with online course participation specifically (Briand et.al., 2023, 2024; Rapisarda et al., 2025). As discussed earlier, digital courses may enable people to gain benefit who might not have been able to attend face to face. This inclusive, preventative approach helps ensure that more people receive the support they need, when and how they need it, reflecting the NHS’s vision of shifting from reactive treatment to proactive prevention and community-based care.
From Analogue to Digital
As highlighted in this briefing paper, Recovery Colleges have been pioneers in digital transformation within health and social care. By adopting online platforms for both enrolment and courses, they demonstrate that digital solutions can complement and enhance traditional in-person services rather than replace them. By introducing online courses, webinars, and streamlined digital enrolment processes, in addition to analogue in person offers, Recovery Colleges can make their support and educational offerings more accessible to a broader audience.
Recovery Colleges could further support digital inclusion by offering courses in digital literacy and to enhance people’s access to other online and digital resources such as how to use the NHS App. They could offer courses and information on how to be online safely or use artificial intelligence (AI) and websites in an informed way, assessing what is good or not so good information.
This digital shift directly supports the NHS’s ambition to modernise and deliver community-centred, digitally enabled care. By leveraging digital technologies, Recovery Colleges break down barriers of geography and accessibility, allowing people to participate in recovery and wellbeing programs from any location.
Reducing the burden on the NHS
In addition to the three key shifts, the 10 year plan for England also highlights the urgent challenge of long waiting lists. Recovery Colleges, particularly through their digital platforms, can offer one practical solution by enabling earlier and broader access to support. Recovery Colleges’ digital and online offers can engage more people more efficiently, providing early intervention that can help reduce demand on waiting lists.
‘Digital Recovery College supports the management of waiting lists by ensuring everyone waiting for an appointment receives information about online webinars, understands what to expect, and has the opportunity to ask questions and consider if an assessment is right for them. In this way, the online RC helps the Trust to manage service pressures.’ (Recovery College Manager, SLaM)
‘Online Recovery College courses are a way we can reach more people even with fewer resources, doing more for less. For example, ten people might attend a course together on understanding and managing their anxiety instead of each seeing a clinician individually. By including clinical leads in co-production, deciding what courses to run, we can help reduce waiting lists.’ (Clinician Trainer, Sussex Recovery College)
Recovery Colleges, especially through their digital and online offers, also support staff wellbeing, giving them opportunities to engage for their own wellbeing and promoting workforce development.
By offering accessible support, Recovery Colleges empower individuals to take proactive steps towards their own well-being while alleviating some of the strain on NHS services, contributing to shorter waiting times and more efficient use of resources.
Conclusions
Recovery Colleges with digital and online offers are uniquely positioned to showcase how we can make the key shifts identified in ‘Fit For The Future, the 10 year health plan for England’, facilitating moves toward prevention and health promotion, community focused approaches, and by definition, from analogue to digital ways of working. They show promising outcomes, and these are likely to be associated with the core features of Recovery Colleges. Online learning has created opportunities for some whilst creating barriers and digital exclusion for others. Access and inclusion have expanded, reaching different communities such as staff, carers and those in rural areas or facing barriers to in-person attendance. It can enable more flexible, individualised learning, allowing students more choice to engage in ways that better suit their needs. It has also strengthened collaboration across Recovery Colleges, supporting the sharing of courses and resources, collective problem-solving, and a more connected recovery education community. However, care needs to be taken to ensure inclusiveness, that Recovery Colleges remain open to all, as some groups experience digital exclusion, including people from already marginalised communities, those facing social disadvantages and people with more serious mental health challenges.
-
Abbasi, M. S., Ahmed, N., Sajjad, B., Alshahrani, A., Saeed, S., Sarfaraz, S., Alhamdan, R. S., Vohra, F., & Abduljabbar, T. (2020). E-Learning perception and satisfaction among health sciences students amid the COVID-19 pandemic. Work, 67(3), 549–556.
Bourne, P., Meddings, S., & Whittington, A. (2018). An evaluation of service use outcomes in a Recovery College. Journal of Mental Health, 27(4), 359–366.
Briand, C., Giguère, C.-É., Macario de Medeiros, J., Vallée, C., Luconi, F., Vachon, B., Drolet, M.-J., Monthuy-Blanc, J., Mahroug, A., & Hakin, R. (2024). The effectiveness of an online short-format Recovery College model: a co-learning model to support mental health. International Journal of Mental Health Systems, 18(1), 17.
Briand, C., Hakin, R., Macario de Medeiros, J., Luconi, F., Vachon, B., Drolet, M.-J., Boivin, A., Vallée, C., & Montminy, S. (2023). Learner experience of an online co-learning model to support mental health during the COVID-19 pandemic: a qualitative study. International Journal of Environmental Research and Public Health, 20(3), 2498.
Briand, C., Vallée, C., Luconi, F., Thériault, J., Sauvageau, A., & Bellemare, J. (2025). State-of-the-art literature review of Recovery College evaluative studies between 2013-2024. Frontiers in Psychiatry, 16, 1584110.
Byrne, D., Martina, T., Sheppard, G., Patmore, L., Howe, M., Senoran Martin, N., Marsh, L., Barnicoat, S., & Meddings, S. (2023, 14.09.23). Sussex Recovery College Ten Year Celebration day 2013-2023 Ten Years Strong.
Crowther, A., Taylor, A., Toney, R., Meddings, S., Whale, T., Jennings, H., Pollock, K., Bates, P., Henderson, C., & Waring, J. (2019). The impact of Recovery Colleges on mental health staff, services and society. Epidemiology and Psychiatric Sciences, 28(5), 481–488.
Department of Health. (2021). Mental health strategy 2021–2031. Department of Health (Northern Ireland). https://www.health-ni.gov.uk/publications/mental-health-strategy-2021-2031
Department of Health and Social Care. (2025). Fit for the future: 10 Year Health Plan for England. London:HMSO. Accessed 10.09.25 from https://www.gov.uk/government/publications/10-year-health-plan-for-england-fit-for-the-future/fit-for-the-future-10-year-health-plan-for-england-executive-summary
Hayes, D., Hunter-Brown, H., Camacho, E., McPhilbin, M., Elliott, R. A., Ronaldson, A., Bakolis, I., Repper, J., Meddings, S., & Stergiopoulos, V. (2023). Organisational and student characteristics, fidelity, funding models, and unit costs of recovery colleges in 28 countries: a cross-sectional survey. The Lancet Psychiatry, 10(10), 768–779.
King, T., & Meddings, S. (2019). Survey identifying commonality across international recovery colleges. Mental Health and Social Inclusion, 23(3), 121–128.
Kotera, Y., Ronaldson, A., Hayes, D., Hunter-Brown, H., McPhilbin, M., Dunnett,
D., Jebara, T., Takhi, S., Masuda, T., & Camacho, E Bakolis I, Repper J, Meddings
S, Stergiopoulos V, Brophy L, De Ruysscher C, Okoliyski M, Kubinová P, Eplov L, Toernes C, Narusson D, Tinland A, Puschner B, Hiltensperger R, Lucchi F, Miyamoto Y, Castelein S, Borg M, Klevan TG, Tan Boon Meng R, Sornchai C, Tiengtom K, Farkas M, Moreland Jones H, Moore E, Butler A, Mpango R, Tse S, Kondor Z, Ryan M, Zuaboni G, Elton D, Grant-Rowles J, McNaughton R, Hanlon C, Harcla C, Vanderplasschen W, Arbour S, Silverstone D, Bejerholm U, Powell C, Ochoa S, Garcia-Franco M, Tolonen J, Yeo C, Charles A, Henderson C, Slade M. (2024). 28-country global study on associations between cultural characteristics and recovery college fidelity. Npj mental health research, 3(1), 46.
Kotera, Y., Ronaldson, A., Takhi, S., Felix, S., Namasaba, M., Lawrence, S., Kellermann, V., Kapka, A., Hayes, D., Dunnett, D., Jebara, T., Murakami, M., Bakolis, I., Repper, J., Meddings, S., Stergiopoulos, V., Brophy, L., De Ruysscher, C., Eplov, L., Toernes, C., Narusson, D., Puschner, B., Hiltensperger, R., Miyamoto, Y., Castelein, S., Klevan, T., Moreland Jones, H., Moore, E., Tse, S., Ryan, M., Zuaboni, G., Hanlon,
C., Asher, L., Vanderplasschen, W., Ochoa, S., Tolonen, J., Charles, A., Andrade, M., Elton, D., Bates, P., Cooper, J., Grant, J., Henderson, C., & Slade, M. (2025). Cultural influences on fidelity components in Recovery Colleges: a study across 28 countries and territories: General Psychiatry; 38:e102010.
McGregor, J., Repper, J., & Brown, H. (2014). “The college is so different from anything I have done”. A study of the characteristics of Nottingham Recovery College. Journal of Mental Health Training, Education and Practice, 9, 3–15.
McPhilbin M, Stepanian K, Yeo C, Elton D, Dunnett D, Jennings H, Hunter-Brown H, Grant-Rowles J, Cooper J, Barrett K, Hamie M, Bates P, McNaughton R, Trickett S, Bishop S, Takhi S, Lawrence S, Kotera Y, Hayes D, Davidson L, Ronaldson A, Jebara T, Hall C, Brophy L, Jepps J, Meddings S, Henderson C, Slade M, Lawrence V. (2024). Investigating the impact of the COVID-19 pandemic on recovery colleges: multi-site qualitative study. British Journal of Psychiatry Open. May 16;10(3):e113. doi: 10.1192/bjo.2024.70. PMID: 38751202; PMCID: PMC11363083.
Meddings, S., McGregor, J., Roeg, W., & Shepherd, G. (2015). Recovery colleges: quality and outcomes. Mental Health and Social Inclusion, 19, 212–221.
Meddings, S., Walsh, L., Patmore, L., McKenzie, K. L. E., & Holmes, S. (2019). To what extent does Sussex Recovery College reflect its community? An equalities and diversity audit. Mental Health and Social Inclusion, 23(3), 136–144.
O’Brien, A., & Forde, C. (2023). Health science staff and student experiences of teaching and assessing clinical skills using digital tools: a qualitative study. Annals of Medicine, 55(2), 2256656.
Patmore, L. (2020). Performance Report (Jan-Aug 2020) - Digital Recovery College - an inaugural summary. Sussex Recovery College.
Perkins, R., Meddings, S., Williams, S., & Repper, J. (2018). Recovery colleges 10 years on. Nottingham: ImROC - Implementing Recovery Through Organisational Change.
Rapisarda, F., Briand, C., Vallée, C., Vachon, B., & Lefay, G. (2025). Clustering change patterns among learners of an online Recovery College in Quebec. Frontiers in psychiatry, 16, 1534349.
Rapisarda, F., de Medeiros, J. M., Briand, C., Boivin, A., Monthuy-Blanc, J., Vallée, C., Drolet, M.-J., Vachon, B., & Luconi, F. (2022). Assessing changes in anxiety, empowerment, stigma and wellbeing in participants attending an Online-Based Recovery College in Quebec during the Covid-19 pandemic: a pre-experimental study. International Journal of Public Health, 67, 1604735.
Richardson, S. (2026). Teaching for Student Success in Vocational Higher Education. London: Palgrave Macmillan.
Ronaldson, A., Allen, T., Bakolis, I., Emsley, R., Jebara, T., Kotera, Y., Dunnett, D., Kaur Takhi, S., McPhilbin, M., Simpson, J., Kapka, A., Killaspy, H., Hayes, D., Namasaba,
M., Meddings, S., Jewell, A., Giles, K., Brophy, L., Shergold, D., Grant-Rowles, J., Bates, P., Elliott, R.A., Henderson, C., Slade, M. (2025 preprint). The impact of Recovery College enrolment on health service use and patient outcomes: retrospective matched cohort study using routinely collected data. medRxiv 2025.12.09.25341905; doi: https://doi.org/10.64898/2025.12.09.25341905
Sauvageau, A., Bellemare, J., & Briand, C. (2025). Learning experience and relationships among learners in online Recovery College courses: An exploratory qualitative study. Journal of Recovery in Mental Health, 8(2), 60–75.
Scottish Government. (2023). Scotland’s mental health and wellbeing strategy. Scottish Government. https://www.gov.scot/publications/mental-health-wellbeing-strategy/
Sussex Recovery College. (2020). Digital Recovery College Project Plan and Description. Sussex Partnership NHS Foundation Trust.
Sussex Recovery College. (2021). Virtual Steering Groups (VSG) Report - Recovery College Winter Term: January - March 2021. Sussex Partnership NHS Foundation Trust.
Sussex Recovery College. (2022). Virtual Steering Group (VSG) Report – Sussex Recovery College Autumn Term: 4 October – 17 December 2021. Sussex Partnership NHS Foundation Trust.
Sussex Recovery College. (various years). Sussex Recovery College Termly Reports. Sussex Partnership NHS Foundation Trust.
Thériault, J., Lord, M.-M., Briand, C., Piat, M., & Meddings, S. (2020). Recovery colleges after a decade of research: a literature review. Psychiatric services, 71(9), 928–940.
Thompson, H., Simonds, L., Barr, S., & Meddings, S. (2021). Recovery colleges: long-term impact and mechanisms of change. Mental Health and Social Inclusion, 25(3), 232–242.
Toney, R., Elton, D., Munday, E., Hamill, K., Crowther, A., Meddings, S., Taylor, A., Henderson, C., Jennings, H., & Waring, J. (2018). Mechanisms of action and outcomes for students in Recovery Colleges. Psychiatric services, 69(12), 1222–1229.
Vallarino, M., Briand, C., Lord, M.-M., & Sauvageau, A. (2026). Logic model for a train-the-trainer program ensuring alignment with recovery college principles and values. Mental Health and Social Inclusion, 30(1), 101–113.
Welsh Government. (2025). Mental health and wellbeing strategy 2025–2035.
Welsh Government. https://www.gov.wales/mental-health-and-wellbeing-
strategy-2025-2035
Wolverson, E., Hague, L., West, J., Teague, B., Fox, C., Birt, L., Mills, R., Rhodes, T., Sams, K., & Moniz-Cook, E. (2024). Building an initial understanding of UK Recovery College dementia courses: a national survey of Recovery College and memory services staff. Working with Older People, 28(2), 108–119.