
When and where does peer support work?
A research lens
Written by Simon Bradstreet
This is the second publication in the demystifying research seriesfrom Imroc.
In the first paper, we explored a deceptively simple question with a less than simple answer.
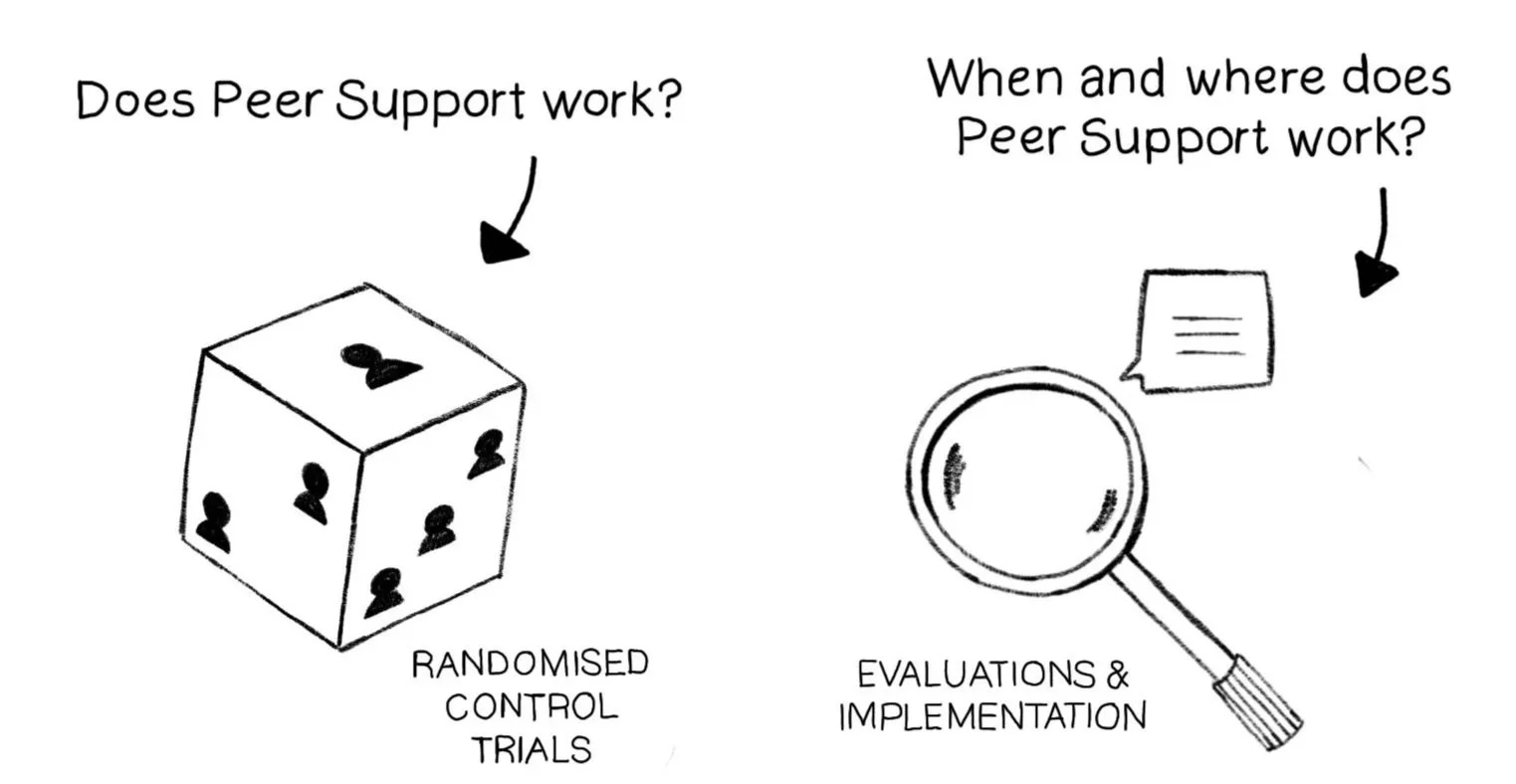
Does peer support work?
In this new paper we continue the focus on research related to peer support and now turn to the question of:
When and where does peer support work?
In unpicking this question, we introduce and explain various research terms in a way which is understandable and accessible. All technical research terms are highlighted and link to our research jargon buster which will grow as we explore more questions and methods.
Because we are now exploring the conditions in which peer support is most likely to be effective and sustainable our attention turns towards implementation research and evaluations.
Summary
This second paper in the demystifying research series explores the question: 'When and where does peer support work?' The paper begins by establishing that while Randomised Controlled Trials, which were the focus of the first paper, can tell us whether peer support works, they tell us little about the conditions that shape its success. For that, we need different approaches. Two types of research are introduced and explained. These are evaluations, which assess whether a programme is working and how it can be improved and implementation studies, which explore the factors that help or hinder the adoption of new approaches in real-world settings. Both tend to draw primarily on qualitative methods, and the paper takes time to explain what qualitative research involves and to address common misconceptions about subjectivity and bias.
Drawing on a 2024 umbrella review, the paper goes on to summarise what the evidence tells us about the conditions for successful peer working. Key factors include co-produced design, recovery-oriented organisational cultures, strong leadership, clear role boundaries, quality training, and appropriate supervision. These findings are consistent across different peer work settings.
The paper concludes with a practical summary table of what to encourage and avoid across the different stages of peer role development. The overall message is clear. We know what good looks like. The challenge lies in making sure it happens.
Let’s recap
The first paper in this series explored the question 'Does peer support work?' We established that, while peer support is not a new phenomenon, formal peer support roles in mental health and related services are. As a result, there has been a great deal of research to test the effectiveness of peer support working.
We introduced Randomised Controlled Trials (RCTs), the primary research method used to test effectiveness and explored why RCTs present challenges when applied to ‘complex interventions’ like peer support. The challenges included variation in what peer support looks like across different studies, inconsistent control conditions, and diverse outcome measures.
Finally, we reviewed what systematic reviews of peer support trials tell us: that peer support working is at least as effective as non-peer delivered alternatives and may be particularly beneficial for recovery-oriented outcomes like empowerment. We also discussed how evidence for impact on clinical outcomes is limited. The quality of studies remains a concern across reviews. (For full details, see paper 1).
OK, so where next?
Randomised Controlled Trials can be helpful in testing whether a tool or approach improves outcomes by running controlled experiments. However, they don’t tell us much about where and when the approach being tested may or may not have an effect.
An RCT might demonstrate that peer support improves certain outcomes - job done, box ticked… but only part of the story. Perhaps that success depended on factors like peer workers having quality supervision and working in a team that respected and understood their role. For those details about when and where things actually work, we need different research approaches.
There are multiple different research methods used to understand the conditions (working contexts, types of peer support roles, length of time offering support etc) in which peer support is most likely to be effective, but in this paper we focus on two:
Programme evaluations
Implementation studies
If you are just interested to know more about what we already know about getting the conditions right for peer support then feel free to jump ahead. If, however, you are here for some more research demystification then read on. :)
What sort of studies are you talking about when you say evaluation and implementation studies?
To get a better sense of the conditions in which peer support is likely to work best researchers inevitably need to speak with the people involved with its design and delivery and ideally also people using peer delivered services. This means the methods used are primarily qualitative. You can read more about qualitative research in the jargon buster but its characteristics include:
It is concerned with experiences, meanings, behaviours, and social phenomena.
Qualitative data is almost always words based and is rarely concerned with numbers (which is the domain of quantitative research).
The focus is on depth and understanding how and why things happen or work and how things are experienced.
Data are gathered using a variety of methods including interviews and focus groups.
Analysis is based on an agreed framework but involves the subjective interpretation of meaning.
Subjective interpretation sounds, well… a bit subjective! What about bias?
Qualitative research is often misunderstood as being inherently biased because it embraces the researcher's own perspective and their subjective interpretation. This differs greatly from quantitative methods where a common aim is to reduce perceived subjectivity through the use of agreed measures and outcomes. However, it’s important to note that subjectivity should not be conflated with bias. Whether we like it or not, all research involves a level of subjectivity.
In qualitative research, the researcher is acknowledged as a research instrument, and their positionality, reflexivity, and transparency about their perspective can actually strengthen the study's credibility rather than compromise it. Good qualitative research employs systematic methods to boost its trustworthiness.
All in, the goal is not to eliminate the human element but to make it explicit and accountable. Once we accept that all research involves human judgment and interpretation, the question becomes less about which method is 'purest' and more about which method is right for the job at hand.
So how do you pick the best research method?
A fundamental principle in research is that the method should align with the research question being considered. If the question seeks to understand lived experiences, meanings, or social processes, all of which apply when exploring the conditions in which peer support is most likely to be effective, then qualitative approaches are not just appropriate but necessary. Quantitative methods don’t help us understand the lived experiences of peer workers or of the people they support. The best way of understanding that is to ask them and then listen to what they have to say!
Which research tells us most about the conditions in which peer support works?
The two types of research that tell us most about the conditions in which peer support is likely to be effective are evaluations and implementation studies, for reasons that will become clear. There is a lot of crossover between these two types of research so let’s look at them one at a time.
Tell me more about evaluations
Evaluation is the systematic assessment of the quality, value, or effectiveness of something, such as a programme, policy or intervention to determine whether it meets its intended goals and objectives. In simpler terms, evaluation is about asking: "Is this working? How well is it working? And how do we know?"
That sounds a lot like research...what's the difference between research and evaluation?
You’re not wrong, evaluation is a lot like research and there is considerable overlap between the terms evaluation and research. There are no hard and fast rules to distinguish them.
Generally speaking, research aims to generate new knowledge, test theories, and contribute to broader understanding that can be generalised to different settings from where the research was done.
Evaluation on the other hand usually aims to assess the merit, worth, or value of a specific programme or intervention in a particular setting to inform practical decisions and improvements. In other words, research asks the big questions; evaluation rolls up its sleeves and checks whether the answers are any use in real life.
Certainly, both involve collecting and analysing evidence to make informed judgments and support decision-making about what to keep, change, or stop, but evaluations tend to be more locally applied and practical and less focused on academia and journal publication.
When do evaluations get done?
Often evaluations are commissioned or carried out when new programmes and projects are developed to help gain an understanding of how it is working and to inform future decision making about the development of a programme. Sometimes evaluations are required by funders or to support good governance within organisations.
Evaluations might take place during the development and implementation of a programme, with learning feeding into its improvement and redesign. This approach to evaluation is described as being formative. In contrast, summative evaluation looks back once a programme has been completed to get a sense of its overall worth.
Sometimes evaluations are embedded within larger research studies to help get a better understanding of how outcomes may or may not have been achieved. These are sometimes described as process evaluations. This type of embedded evaluation is concerned with questions like:
What actually happened?
Was the program delivered as planned (also known as fidelity)?
Why did it work (or not work) in this setting?
What would we need to replicate this elsewhere?
Combining evaluation findings with outcome data can give a richer understanding of how outcomes were, or were not, achieved in quantitative studies like Randomised Controlled Trials.
Combining learning from qualitative evaluation with findings from quantitative methods like RCTs is known as applying mixed methods and is widely encouraged in research guidelines and by funders.
What is implementation?
Implementation is the process of putting a plan into action to include evidence-based practices as part of routine care and support. Having evidence for an approach does not necessarily mean it will be adopted without careful consideration of the barriers and facilitators for adoption and having a plan to address them.
What is known as Implementation Science developed in response to the slow uptake of evidence based approaches in health and care settings. It’s a much-needed area of research, based on what we know about how long it takes research evidence to begin to influence the way we practice. One widely cited study suggested it takes an average of 17 years for just 14% of original research findings to be implemented into routine clinical practice in health settings (Balas & Boren, 2000). If you apply that to the peer support research, that means that some of the earliest studies of peer support practice in the UK are still a couple of years away from influencing the day to day practice of introducing peer support in mental health services. That's not great for our peer support context but looks like 2043’s going to be an amazing year for peer support!

Implementation frameworks like CFIR and RE-AIM are often used in this type of research. They serve as structured guides for understanding why interventions succeed or fail when moved from research into real-world settings.
Frameworks can also be used to guide the planning and development of projects. A team introducing peer workers to a crisis service might use an implementation framework to help them anticipate barriers (perhaps staff attitudes, or lack of appropriate supervision structures) and facilitators (strong leadership support, existing recovery-oriented culture). This helps them design their approach and anticipate challenges with an evidence-based approach.
There are a great many of these frameworks. So many that some have commented that they are a bit like toothbrushes… nobody wants to use someone else’s, so they make their own!

So, if they’re both important, do evaluation and implementation link?
Implementation is about the doing, in our case putting peer support into practice in a particular setting. Evaluation is about learning, which means finding out whether it's working and why. You need both, and they inform each other.
Think of an organisation introducing peer workers for the first time. Implementation would involve all the practical steps from planning to recruiting peer workers, training them and the wider team, finding them a place in existing structures, and addressing barriers as they arise. Evaluation would ask: Is this working? Are people benefiting? What's helping or hindering? The learning from that evaluation feeds back into implementation and creates a cycle of doing, learning, and improving.
In research, these two areas often overlap. Many evaluations of peer support address implementation questions (exploring barriers and facilitators) without necessarily using formal implementation frameworks.
OK, I’m starting to understand what evaluation and implementation research are... so what do they tell us about the conditions in which peer support works?
There have been too many evaluations and implementation studies of peer support to summarise them all here, but thankfully other people have attempted to do just that (more of which later).
To make things simpler we have summarised findings from across all the studies mentioned in this paper into one table, which breaks down findings by the stage of peer worker role development.
A challenge is that many evaluations are not journal published because they have been developed in services or organisations. This means their findings are mainly aimed at improving those services and are not necessarily widely shared.
Publishing in journals isn’t the only way knowledge travels, but it does stop valuable learning staying stuck in a filing cabinet somewhere. The type of publication that isn’t published in an academic journal, but still has academic relevance is rather gloomily referred to as grey literature. You might be picturing cobwebs, but their greyness does not mean they are boring or of less value than journal published findings. It does mean they have not been subject independent peer review before publication.
We already mentioned that other people have attempted to summarise findings from evaluations (lucky for us...) so, to make things manageable in this paper, we will focus on evidence from systematic and umbrella reviews to summarise evidence for the conditions in which peer support works.
Systematic...umbrellas? I need a reminder…
Remember systematic reviews from the first paper in the series? They're often used to inform decision making in health and care settings. They gather all the relevant studies in an area, evaluating their quality, and synthesising findings. Umbrella reviews work in a similar way, but with one key difference. While systematic reviews analyse individual research papers, umbrella reviews zoom out one level further - they review and draw conclusions across previous systematic reviews.
All in, their findings are a good place for us to start.
What are the headlines?
A 2024 umbrella review considered evidence from nine systematic reviews (Cooper et al., 2024), all of which included evidence about the conditions for successful peer working. You might remember this review from part one of this series where we focused on its findings about the effectiveness of peer working. The effectiveness of peer working was one of three questions in the review.
The second and third questions set in the review are directly relevant to our exploration of the conditions for successful peer working:
What influences the implementation of peer support approaches for mental health?
What are the experiences of peer support approaches for mental health (e.g. of acceptability) from the perspective of peer support workers (PSWs), healthcare practitioners, people using services and carers?
Let’s look at what they found.
Finally...tell us! What influences the implementation of peer support approaches for mental health?
Umbrella review findings were presented against five headings derived from the Consolidated Framework for Implementation Research (CFIR: Damschroder et al., 2009).
These headings represent the things which are known to be important for successful implementation in real world settings:
Innovation (the ‘thing’ being implemented)
Outer setting (the setting in which the inner setting exists, for example. a healthcare system)
Inner setting (the setting in which the innovation is being implemented, for example a service or team)
Individuals (the roles and characteristics of people involved)
Implementation process (the activities and strategies used to implement the innovation).
The umbrella review found that successful implementation of peer support in mental health settings depended on factors operating at different levels. At the broadest level, national policies supporting peer worker employment, integration within health and care systems, and access to peer networks all helped, while medical model dominance and a lack of recognised certification created system-wide barriers.
Within organisations, strong leadership, recovery-oriented cultures, and practical resources for peer workers were essential, with time pressures, inadequate pay, and organisational resistance working against success. The design of peer support itself mattered too, with co-produced and collaboratively developed approaches proving more effective than those imposed from outside.
The people involved, peer workers, their colleagues, and organisational champions mattered. Rigorous recruitment, quality training linked to professional standards, and genuine staff acceptance of peer workers as colleagues were all identified as important facilitators.
Finally, how peer support was put into practice proved as important as the conditions surrounding it. Ongoing supervision, clear role boundaries, wellbeing safeguards, and thoughtful matching of peer workers to the people they supported all contributed to whether peer support flourished.
The authors of the umbrella review concluded (page 42):
“Good implementation of peer support depends on co-design with people with lived experience, clear job descriptions, a recovery-oriented workplace culture, strong leadership, appropriate training for PSWs and staff, and supervision for PSWs.”
But what do peer support workers themselves think?
The third question of the umbrella review focused on the experiences of peer support approaches from different perspectives, including peer workers wider staff and people using peer provided services. Drawing findings from eleven included reviews, three high level themes were identified across different groups:
What the peer worker role can bring.
Confusion over the role.
Organisational challenges and impacts.
Focusing on the views of peer support workers, a number of benefits of being in the role were identified. These included:
Benefits for peer workers themselves, including improved self-esteem, greater self-acceptance and enhanced recovery.
The role can therefore be mutually beneficial.
Peer workers can role model recovery, sharing hope.
However, the role can also affect Peer Worker’s sense of self, their general wellbeing and recovery, so comes with personal risks.
To supplement this evidence the same research team completed new research to explore the barriers and facilitators to delivering peer support effectively from the perspective of peer support workers who were based in England (Foye et al., 2025).
Findings were in line with the umbrella review in that the peer workers highlighted the importance of supervision and training and of working in teams who value and understand peer support. They also highlighted the need for peer working practice to be flexible and adaptable to different peer interactions. However, at the same time peer working also needs to take place within agreed boundaries.
Managing the complexity of peer working within established health care settings was challenging and barriers to progression and role recognition made this harder to manage.
Most of the research seems to be about peer working in health systems – what about community and voluntary sector based peer working?
You're right to notice this. Journal published research has a strong bias towards peer working in statutory health settings. This reflects broader patterns in research rather than where peer support actually happens. Various forms of peer support are common across voluntary, community and social enterprise (VCSE) settings, and there is important evidence to draw on from these contexts even if it is less visible in academic literature.
Some key points of learning from VCSE based peer support literature:
VCSE organisations are well placed to sustain the principles and ethos of peer support, especially in the early stages of developing roles, through training and supervision rooted in peer values (Faulkner, 2020).
Partnership models, where VCSE employed peer workers are embedded in statutory health settings can have advantages (Repper et al., 2021) and with thoughtful collaboration and support can lead to positive outcomes (Bradstreet & Cook, 2021).
Evidence from Rethink’s internal evaluation echoes wider findings about the value and unique contribution of peer workers in VCSE settings, while also reinforcing the messages about the importance of role clarity, appropriate support and training, and careful thinking about the purpose and goals of peer working in any new development (Moran, 2023).
VCSE organisations should not be viewed as a cheaper delivery option but should be commissioned on the basis of their proven knowledge, expertise and skills in peer support (Faulkner, 2020).
Taken together, this suggests the question is less about whether VCSE-based peer working is effective and more about the conditions needed to make it work well. Those conditions turn out to be remarkably consistent across settings.
What should we take from the evidence overall?
The formalised peer support worker role is unique and complex. No other role asks people to build their practice from their own lived experience. We now have clear evidence that peer support brings distinct benefits to people using peer services. However, we also know that peer workers face risks when working in inappropriate settings or without adequate support. These risks extend to the people they work with, though typically to a lesser degree.
The good news is that we understand what needs to happen to maximise the benefits while minimising the risks. This is based on a well-established and consistent evidence base.
There are numerous publications and guidelines available to encourage the thoughtful development of peer support worker roles including those developed by Imroc and anyone developing peer roles is encouraged to explore them. Meantime the following gives a summary of what we know from published evidence about how to create the conditions for successful peer working.
The following table, which is based on findings of studies mentioned in this paper, makes recommendations around what to encourage and what to avoid when developing or maintaining peer roles. These are broken down by the stage of peer role development.
| Stage | ✓ Encourage | ✗ Avoid |
|---|---|---|
| Planning and development | Co-produced approaches where people with lived experience are involved in all stages of design and planning. | Top-down approaches that do not engage with all stakeholder groups including peers. |
| Identifying recovery-oriented, welcoming and understanding settings and teams. | Seeing peer workers as a means of shifting unhelpful cultures or saving money. | |
| Identifying the right place in teams and systems for peer workers to be effective, with leadership support. | Assuming peer workers can be effective in any setting and for achieving any outcome. | |
| Ensuring appropriate office space and equipment as well as access to necessary records and systems. Taking time to orient peer workers to team processes. | Treating peer workers as visitors rather than members of the team. | |
| Team preparation to raise awareness of peer working and support role clarity. | Assuming wider teams welcome or understand the role and its fit. | |
| Partnership approaches are based on a genuine assessment of what partners bring to peer roles and on thoughtful collaboration. | Seeing VCSE providers of peer workers as a cheap option, or a way of outsourcing the difficult bits of introducing peer workers. | |
| Refer to evidence and implementation guidelines. | Assuming that developing peer roles will be like any service development. | |
| Codes of practice and values base for peer roles and practices are identified and understood. | Adopting values and practice guidelines from other professions. | |
| Identify and support champions and leaders who advocate for peer working. | Relying on the enthusiasm of one or two individuals without embedding support for peer working across leadership and teams. | |
| Recruitment and startup | Role and its competencies are clearly described during recruitment with salary positioned to reflect any national standards. | Shoe horning peer worker role descriptions and specifications into existing documents. |
| Communication with Human Resource and Occupational Health teams to describe the role and ensure recruitment is supported. | Assuming HR and Occupational Health teams understand peer support or are well versed in supporting people with lived experience into professional roles. | |
| Rigorous recruitment processes that are sensitive to where people are in their recovery. | Requiring 'recovered' status for peer roles or setting arbitrary timescales for applicants to have been discharged/out of treatment before they can apply. | |
| Appropriate and, where available, certified peer worker training is available. | Failing to provide recognised training specific to the role. | |
| Processes for planning wellness at work for peer workers including crisis planning and occupational health support if available. | Making assumptions that peer workers do not want support or adjustments. Conversations about wellbeing eclipsing the peer workers abilities and strengths. | |
| Considering how peer workers are matched with people they might support to enhance connection. | One-size-fits-all allocation that ignores the preferences and characteristics on both sides. | |
| In post | Specific peer supervision and support with appropriate supervisors. Consider offering more supervision for peer workers as they settle into roles and identifying a team member to act as a mentor and offer informal support. | Providing standard/generic supervision which is not peer informed. |
| Attention to safeguarding for peer workers including review of 'triggering' context/settings. | Avoiding exposing conversations about wellbeing with peer workers. | |
| Build in safe ways to monitor and evaluate role clarity, fit, integration and impact. | Failing to build on or reflect on learning. Failing to address areas of practice where peer workers might develop further. | |
| Opportunities for constructive and continual communication between peer workers and non-peer colleagues. | Allowing poor communication or isolation of peer workers from the wider team to go unaddressed. | |
| Striking a balance between flexible peer practice that adapts to each relationship and the need for structure. | Role drift, because of role ambiguity or a lack of structure or practice guidance. | |
| Allow space for reflection and learning on role identity boundaries and development. | Expecting peer workers to navigate identity tensions without support. | |
| Creating access to other peer workers in group supervision or informal support spaces to reduce isolation, affirm peer identity and encourage shared learning. | Employing a single peer worker or peer workers in disparate teams with no peer network to access. | |
| Moving on and up | Opportunities for progression, both in terms of higher pay, and in terms of expanding skill sets are available. | A ceiling for peer workers roles. |
| Opportunities for the extension and development of peer-based services. | Systemic barriers including a lack of funding, strategic or policy support. |
Conclusion
Getting peer support right requires attention at every stage, from initial planning through to long-term career development. The evidence consistently points to thoughtful planning, appropriate training and supervision and sustained organisational commitment. The challenge isn't knowing what to do. It is perhaps more about making sure it happens.
In exploring that evidence, this paper has introduced a range of research approaches that go beyond the RCTs we focused on in the first paper. Qualitative methods, evaluations and implementation studies each bring something different to our understanding, not just whether peer support works, but under what conditions, for whom, and how to make it stick.
No single method has all the answers, and the strongest evidence base draws on multiple approaches. As with the first paper in this series, the message is not simply to trust research findings at face value, but to engage with them critically: asking who did the research, how it was done, and what it can and cannot tell us.
-
Balas, E. A., & Boren, S. A. (2000). Managing Clinical Knowledge for Health Care Improvement. Yearbook of Medical Informatics, (1), 65–70.
Bradstreet, S., & Cook, A. (2021). Evaluation of the Peer Support Test of Change. Matter of Focus.
Cooper, R. E., Saunders, K. R. K., Greenburgh, A., Shah, P., Appleton, R., Machin, K., Jeynes, T., Barnett, P., Allan, S. M., Griffiths, J., Stuart, R., Mitchell, L., Chipp, B., Jeffreys, S., Lloyd-Evans, B., Simpson, A., & Johnson, S. (2024). The effectiveness, implementation, and experiences of peer support approaches for mental health: a systematic umbrella review. BMC Medicine, 22(1). https://doi.org/10.1186/s12916-024-03260-y
Damschroder, L. J., Aron, D. C., Keith, R. E., Kirsh, S. R., Alexander, J. A., & Lowery, J. C. (2009). Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implementation Science, 4(1), 1–15. https://doi.org/10.1186/1748-5908-4-50
Faulkner, A. (2020). Peer-Support-working-with-the-VCSE-sector. https://amhp.org.uk/peer-support-working-with-the-vcse-sector/
Foye, U., Lyons, N., Shah, P., Mitchell, L., Machin, K., Chipp, B., Jeffreys, S., Jeynes, T., Persaud, K., Nicholls, V., Cooper, R. E., Grundy, A., Pemovska, T., Ahmed, N., Appleton, R., Repper, J., Johnson, S., Lloyd-Evans, B., & Simpson, A. (2025). Understanding the barriers and facilitators to delivering peer support effectively in England: a qualitative interview study. BMC Psychiatry, 25(1). https://doi.org/10.1186/s12888-025-06850-z
Moran, R. (2023). Peer Support Workers: Exploring Rethink Mental Illness’s Practice. https://www.rethink.org/media/6961/peer-support-workers-at-rethink-mental-illness-exploring-our-practice-full-report.pdf
Repper, J., Walker, L., Skinner, S., & Ball, M. (2021). Preparing Organisations for Peer Support: Creating a Culture and Context in which peer support workers thrive. https://www.imroc.org/publications/preparing-organisations-for-peer-support-creating-a-culture-context-in-which-peer-support-workers-thrive